1) Weight gain
Weight gain is an obvious change during pregnancy. Women may lose weight
especially in the first trimester due to vomiting and nausea. However the overall
pattern is weight gain. The amount of weight gained and composition are major
determinants of the extra energy and nutrient needs. The weight gained is also a
determinant of birth weight. Weight should be monitored throughout pregnancy and
therefore, the baseline measurement should be taken. Adequate weight gain is
essential for foetal growth and desired weight gain is based upon pre -pregnancy
weight using BMI criteria and pre-conceptual nutritional status of the woman.
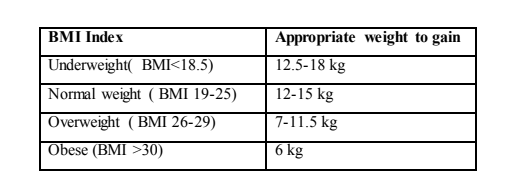
Underweight women are advised to gain more weight during pregnancy to avoid
giving birth to pre-term and low birth weight babies while overweight women are
advised to limit weight gain during pregnancy, Table 9.1. However, pregnancy should
not be used as a time for weight loss.
Table 9.1: Desired weight gain during pregnancy
Maternal size is a conditioning factor on the ultimate size of the placenta. The size of
the placenta determines the amount of nutrition big mothers tend to have big babies
and it is proposed that available to the foetus.
Of the total weight gain, 62% is water, 10% is an increase in blood volume, 13% is
extracellular fluid, 30% is fat and 8% is protein. Adipose tissue accumulate more
128
rapidly in mid pregnancy and the most marked increases in body fat occurs in the
abdominal, subscapular and upper thigh. The foetus accounts for approximately 25%
of the total weight gained, but for only 10% of the total fat stored but 60% of the total
protein gained in foetus and placental tissues. The adipose tissue stored during early
pregnancy is available to meet the needs for foetal growth in the last trimester and
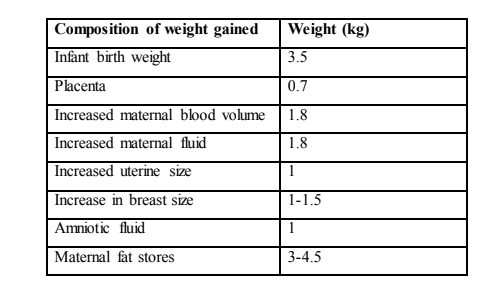
increased energy needs of lactation, Table 9.2.
Table 9.2: Average distribution of weight gain during pregnancy
2) Blood volume and composition
Increases in total blood plasma volume are approximately 33% above normal levels
and may increase to 50% by the end of pregnancy especially in primiparas or in
multiparas. This increases move blood to circulate through the placenta to carry
nutrients to the foetus and carry metabolic wastes. Red cell mass increases only by
15-20% causing haemodilution and therefore the haemoglobin and hematocrit
concentration decrease especially during the second and third trimester when the
largest rise in plasma blood volume occurs. Albumin and water soluble vitamins
increase but per volume value drops. The level of most globulins, lipids and free fatty
acids increase in concentration.
3) Cardiovascular and pulmonary changes
In most women blood pressure decreases during the first and second trimesters due to
peripheral vasodilation but returns to normal in the third trimester. To provide
increase cardiac output slight cardiac hypertrophy (increase in size of the cardiac
muscles leading to high pressure) occurs with increased pulse rate. Maternal oxygen
requirements increases and the threshold for carbon dioxide are lowered making the
pregnant woman feel dyspneic (shortness of breath) with an increased need to
breath. The growing foetus also pushes the diaphragm upwards making breathing
difficult. However there is more efficient gas exchange in the lungs at this time.
4) Gastrointestinal changes
There is a decrease in gastric motility and intestinal tone. This slows down passage of
food through the gastrointestinal tract and enhances absorption of nutrients. On the
other hand decreased motility and crowding of the abdomen with the foetus
causes constipation. A relaxed lower oesophageal sphincter leads to regurgitation
causing heartburn. Intestinal secretions such as hydrochloric acid are decreased
reducing acidity and depress iron and calcium absorption but this is counter
balanced by other factors in the third trimester such as increased uptake of iodine by
the thyroid.
5) Renal changes
Renal plasma flow increases by 75% and glomerular filtration rate by 50%,
accompanied by a greater urinary excretion of glucose, amino acids and water soluble
vitamins. The kidney is not able to adjust completely hence nutrients that would have
been otherwise re-absorbed are excreted. The ability to excrete water is lowered and
the presence of mild oedema is normal except when it is associated with pre-eclamsia
(hypertension and proteinuria).
Titany answered the question on
November 8, 2021 at 06:42